Nearly half of U.S. primary care physicians report burnout — one of the highest rates among high-income countries — and administrative burden is the top reason. Primary care physicians (PCPs) would need to work nearly 27 hours per day to complete all recommended care and administrative tasks, and it’s costing the system $260 million annually in turnover alone. More physicians are leaving. And the patients who depend on them most are being left without a front door into the healthcare system.
At Insight Partners, we believe the cycle of increasing resources with steady, suboptimal outcomes must end. AI, used thoughtfully by PCPs, is a powerful lever. Paired with creative care delivery models, AI offers the greatest hope for stronger outcomes, lower costs, and excellent care regardless of socioeconomic background or geography.
The cost of healthcare is rising, yet outcomes are not improving
U.S. health insurance premiums have skyrocketed over the past 30 years, growing around 6% annually, far outpacing inflation and wage growth, but outcomes have remained mixed. For example, while mortality rates from chronic illness have decreased, life expectancy has stagnated, and chronic illness prevalence has increased. The U.S. has the lowest life expectancy, the highest maternal mortality, and higher admissions for chronic ailments compared to peer nations. The U.S. does lead, however, in the ability to treat many chronic illnesses, such as cardiovascular emergencies and post-operative complications.
As healthcare spending rises, population health is not improving — only our ability to treat late-stage chronic illness.
Why is this the case?
A primary care system stretched to its limits
The primary care crisis isn’t just a supply-and-demand mismatch — it’s the product of decades of structural choices. The way physicians are trained, paid, and asked to practice has made primary care an untenable career, even as the need for it grows.
More patients, same system
Demand for primary care in the U.S. is outpacing supply — driven by an aging population, a more health-conscious public, and a healthcare system that increasingly routes everything through a single front door.
The numbers tell the story. Average new patient wait times have surged from around 20 days in the early 2000s to over a month in 2025 as demand for care has skyrocketed and physician supply has lagged. But the wait time is a symptom, not the cause. Three converging forces are driving the pressure.
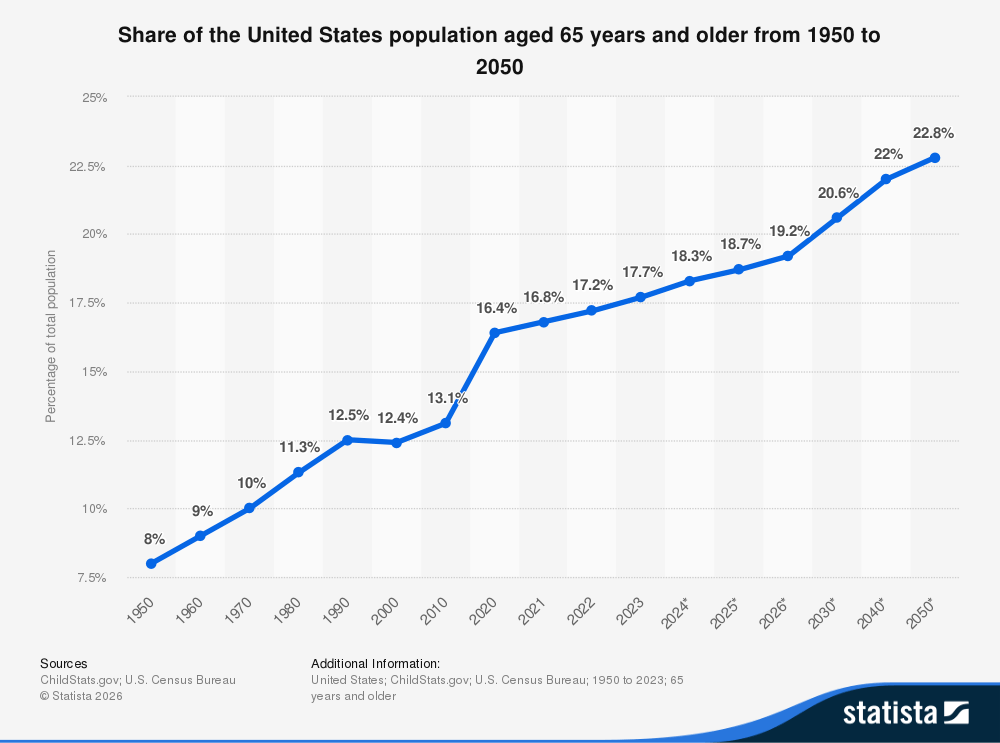
The first is demographic. The U.S. population is aging rapidly, with Baby Boomers driving a significant increase in the number of Americans aged 65 and older. Older patients often live with multiple chronic conditions, see specialists more frequently, and need more from their primary care providers — placing real strain on a system that’s already stretched thin.
The second is behavioral. Rising health literacy, direct-to-consumer healthcare advertising, and the proliferation of consumer health information online have led patients to be more proactive in seeking care. Preventative screenings, mental health services, and chronic disease management have all seen increased utilization as awareness grows, expanding the demand placed on PCPs who serve as the entry point to the system.
The third is structural, and in many ways the most stubborn. As medicine has become more specialized, PCPs have often become referral coordinators rather than comprehensive care providers. Each visit often generates follow-up referrals, additional testing, and return appointments—a self-reinforcing cycle that multiplies patient touchpoints and amplifies the pressure from the first two forces.
Why fewer doctors are choosing primary care
If the demand side of the primary care crisis is about more patients needing more care, the supply side is about a profession that has made itself increasingly hard to enter — and harder to stay in.
The most visible pressure is burnout. Physician shortages are driven by PCPs retiring early and leaving medicine altogether, as administrative burden crowds out the work that drew most physicians to the field in the first place. Almost half of clinicians report burnout tied to tasks like electronic health records (EHRs) and prior authorization management — work that has little to do with patient care. The consequences are stark: 40% of PCPs are considering leaving medicine, and 80% of internal medicine residents are choosing to subspecialize rather than enter primary care.
But burnout alone doesn’t explain why fewer physicians are choosing primary care in the first place. The economics don’t add up. Medical school debt has ballooned to over $200,000, up from around $90,000 in 2000, while inflation-adjusted primary care salaries have declined over the same period. For a medical student doing the math, primary care is underpaid relative to the value it creates in prevention, cost containment, and longitudinal patient relationships.
And even for those who want to enter primary care, the pipeline itself is constrained. Medicare, under the Balanced Budget Act of 1997, largely funds residency positions, capping the number of training slots available regardless of demand. In 2026, there were nearly 6,500 more medical school graduates than available residency positions — a structural ceiling on how quickly the workforce can grow.
The result is a profession being squeezed from every direction: Too much administrative burden for those already practicing, too little financial incentive for those considering it, and a training pipeline that can’t scale to meet the need. We believe the most viable path forward is equipping the physicians we have with AI tools that enable them to do more — risk-stratify patients, support diagnosis, and coordinate care — without adding to their workload.
Fee-for-service models can create misaligned incentives
Fee-for-service (FFS) models have dominated healthcare reimbursement since the 1930s. The premise is simple: Providers are paid a negotiated rate for delivering episodic healthcare services. The result has been a system optimized for doing more — more procedures, more interventions, more billable visits — often, at the expense of keeping patients healthy in the first place. PCPs see 20 to 30 patients per day, with each getting only around 15 to 20 minutes of their doctor’s time, and limited innovation in population health screening and care coordination technologies.
The shift to value-based care
Value-based care (VBC) emerged from the shortcomings of FFS and was implemented nationally through the Affordable Care Act (ACA 2012) and the Medicare Access and CHIP Reauthorization Act (MACRA 2015). The ACA introduced outcome-based payment models through multiple programs, including Hospital Value-Based Purchasing (VBP), HAC Reduction (HACRP), Readmissions Reduction (HRRP), and Medicare Shared Savings (MSSP) — all designed to reward quality and cost reduction rather than service volume.
The Centers for Medicare and Medicaid Services (CMS) deployed these programs gradually, driving recent innovation across three phases:
Measurement
Initial programs had low penalties and bonus potential for quality metric reporting and basic performance benchmarks. For example, HRRP began with a 1% penalty in 2013 for hospitals and new accountable care organizations (ACOs). With light financial incentives tied to quality-of-care reporting, hospitals adopted technologies to provide unified views of their patients, leading to companies such as Innovaccer and Datavant that link longitudinal patient records across providers and payers.
Management
As penalties grew to 3% over time and downside risk was introduced to both ACOs and individual providers through MACRA, focus shifted to improving care quality and closing care gaps through better coordination. This need led to the success of companies such as Aledade, making ACO participation easy while closing care gaps.
Prevention
With reporting infrastructure maturing and quality benchmarks tightening, systems now face pressure to prevent chronic disease rather than just manage it. Companies like Cadence Care embed remote patient monitoring into health system workflows to proactively manage patients with chronic diseases between visits.
Each phase of financial pressure has unlocked a new layer of the care management technology stack — from infrastructure, to coordination, to prevention.
CMS hasn’t stopped pushing. The ACCESS Model represents its most direct move yet toward paying for outcomes rather than visits. VBC arrangements are increasingly focused on innovation in prevention, prioritizing technologies that can identify and proactively manage chronic conditions.
How AI expands what primary care physicians can do
Value-based care has meaningfully shifted the financial logic around prevention, but better reimbursement doesn’t fix a primary care practice’s day-to-day issues. AI’s ability to automate administrative burden and coordinate care addresses this gap in ways previously not possible.
We see the purview of primary care expanding over time as diagnostic technologies democratize, enabling PCPs to perform tech-enabled triage and minor procedures once reserved for specialists. The result is a system where both PCPs and specialists spend more time practicing at the top of their licenses.
Advanced screening technologies enable PCPs to catch disease earlier and more holistically
PCPs are often the first to see a patient before a disease develops. The problem is that they rarely have the technology to catch it. New technology deployed in the primary care setting will help PCPs measure nuanced biomarkers and screen and evaluate patients more comprehensively. When the right tools reach primary care, physicians can catch what they would otherwise miss, while specialists can focus on the patients who need them most.
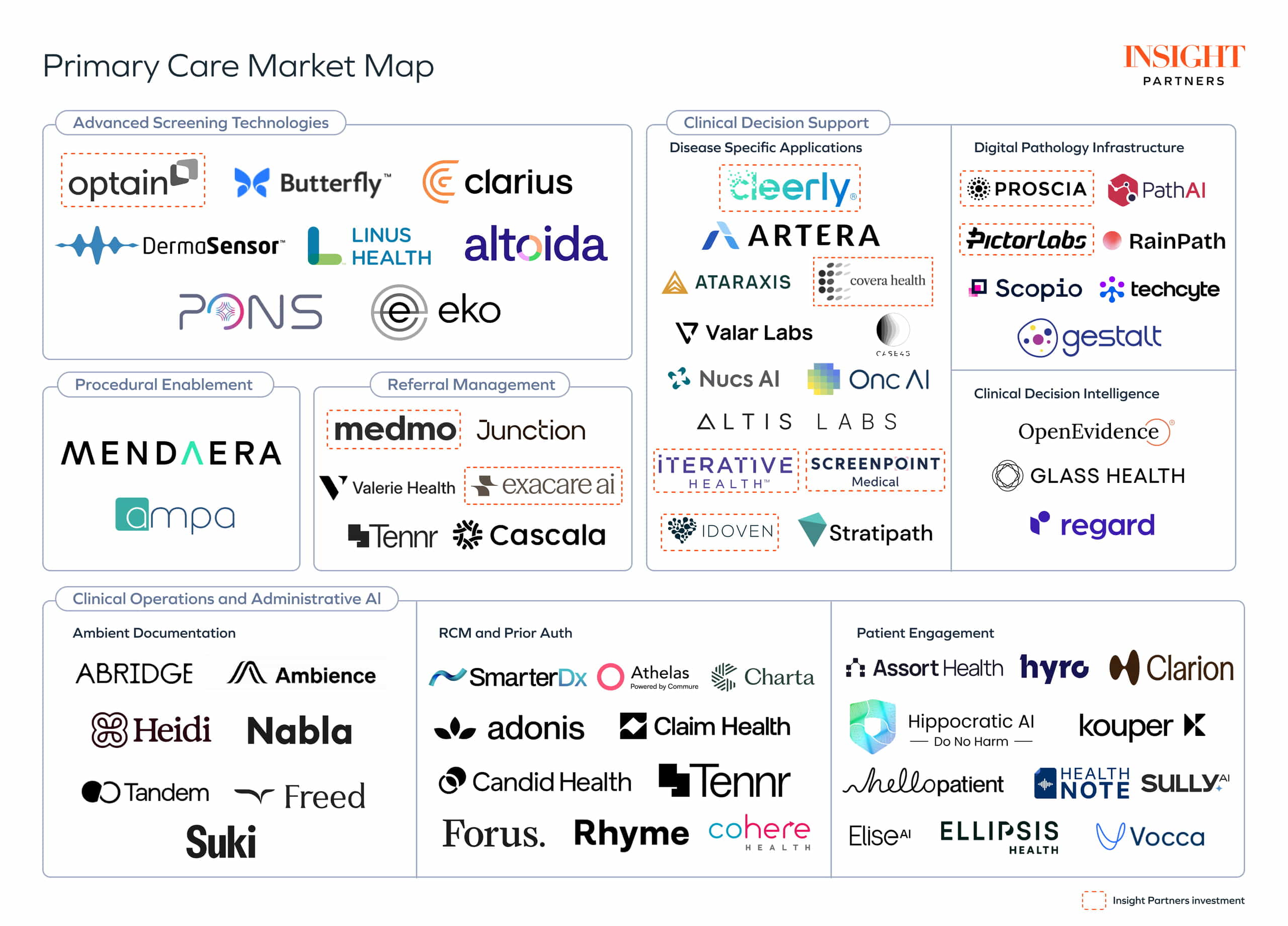
Novel measurement modalities will likely be a key enabler for PCPs to track and quantify biomarkers. Companies such as Dermasensor, which enables PCPs to visualize and evaluate skin lesions, and Optain Health*, which allows PCPs to screen for diseases such as diabetic retinopathy, are two examples of these technologies. Each can be used at the PCP level to catch disease earlier, enrich referral pipelines, and free up specialist time to focus on higher-severity, more complex patients.
Referral management
Better diagnostics can improve efficiency if patients follow up with the right specialists, but unfortunately, up to 50% of subspecialist referrals are never completed. The referral journey is riddled with failure points, including:
- Difficulty identifying accessible in-network specialists
- Referrals lost over fax or through incomplete EHR transmissions
- Inadequate upfront severity triage
- Patients left to self-schedule
- Pre-visit coordination gaps that cause appointment rescheduling
- Specialists rarely close the loop back to the referring PCP
The result is fragmented, uncoordinated care that often leaves the most at-risk patients falling through the cracks. New companies and technologies are necessary to automate, coordinate, and streamline the delivery of clinical care in our currently fragmented care delivery system. Companies such as Medmo*, which automates end-to-end radiology referral management, and Junction, which automates blood-work and diagnostic testing management, are enabling broader follow-through to diagnostic care.
Enablement of procedures in the PCP Office
Most minor procedures PCPs could perform are currently done in specialist offices or hospital outpatient departments. Often, these procedures come at a higher cost and with longer wait times. There are many historical reasons for this, including training, physician comfort, and lack of appropriate setting or equipment. Enabling PCPs to perform these procedures can improve patient access, relieve specialist backlogs, and increase PCP revenue.
Innovation here involves affordable, AI-guided procedural devices that bring specialist-level capabilities to primary care. Companies like Butterfly and Clarius are democratizing point-of-care ultrasound; Mendaera is enabling AI-guided needle procedures such as joint injections and biopsies to be performed semi-autonomously; and Ampa is expanding neuropsychiatric access through AI-guided transcranial magnetic stimulation (TMS) without specialist administration.
Clinical decision support (CDS) and predictive analytics
Two converging trends have made clinical decision support (CDS) newly viable. Health records are now largely digital, and the cost of genomic sequencing has fallen from over $10 million per genome in 2005 to under $1,000 today — creating rich, longitudinal datasets that didn’t exist a decade ago. The patterns buried in that data, when surfaced correctly, can meaningfully change how chronic disease is identified and treated.
The most mature application so far is precision oncology, where EHR, multi-omic, and histopathological data are increasingly used in everyday treatment planning. The core value is straightforward: Help clinicians sub-stratify disease and predict how a patient will respond to treatment before committing to it. We see some of the greatest opportunities in two areas: the underlying data infrastructure that enables this, and disease-specific applications built on top of it.
Most CDS platforms for initial disease profiling require a biopsy and tissue digitization to analyze morphological and/or inferred genetic biomarkers. Pathologists have historically worked manually; therefore, the digitization of pathology is a key unlock. Companies like Pictor Labs* enable virtual staining from a single tissue sample, eliminating the need for multiple biopsies to run different tests, while companies like Proscia* are shifting tissue analysis workflows online.
CDS platforms are increasingly feasible as technology advances and physicians expand their use across their patient populations. Companies like Covera Health* optimize imaging and care pathways for patients whose diagnoses often goes untreated. Concurrently, major biopharma companies are using this technology across clinical trial pathways, including CDS platforms to predict drug success in their pipelines and minimal residual disease (MRD) testing as an endpoint in clinical trials. Tempus is building large suites of patient testing and stratification tools, while companies like Artera and Ataraxis are developing disease-specific models for prostate and breast cancer.
Automation of clinical and administrative tasks
The past decade has seen an ongoing increase in the administrative burden on PCPs, including EHR tasks and prior authorization management. The digitization of the electronic record has, counterintuitively, increased the documentation burden on PCPs, a problem that agentic systems are well-positioned to solve.
AI scribes have seen success with companies such as Abridge and Ambience Healthcare, experiencing some of the fastest healthcare technology adoption to date. And scribing is only the start. The administrative layer is attracting a new generation of purpose-built tools: Tennr for prior authorization, SmarterDx for revenue cycle management, and Assort and Hyro for scheduling and front office automation.
Agentic AI has helped slow the growing administrative burden, sapping physicians’ time and resources from patient care. As reimbursement rates continue to stagnate while administrative duties increase, the economics of independent practice are increasingly degrading. The burden relief will continue to help physicians maintain independence and devote more time to their patients.
Considerations for founders
Below are a few considerations we recommend for founders building businesses to empower PCPs:
Immediate value creation
Primary care clinics are generally low-margin and face mounting payroll, technology, and supply costs while reimbursement rates remain flat or decrease. Therefore, it is crucial that new tools deliver immediate, tangible value to PCPs. Founders should ask themselves, “How do we increase the quality of care while increasing revenue or decreasing non-clinical burden for PCPs?”
Many AI-assisted screening tools struggle to achieve incremental reimbursement because policymakers rely on higher patient throughput to drive ROI. Increased volume can be a strong enough incentive for specialists to adopt new tools, but PCPs often need incremental reimbursement to adopt. Retinal screening is a rare example of a policy already in place for incremental reimbursement.
Speed and workflow
Physician workflows are heavily ingrained due to years of training and optimization. Products that add steps to workflows are likely to fail from the start, whether that’s opening multiple new windows in the EHR or performing lengthy additional tests. Enabling non-clinical staff to perform testing or adding tests to PCP routines without adding to workflow is crucial to ensure adoption and ROI.
Practicing within scope and referral relationships
PCPs and specialists maintain referral networks built on mutual trust, with specialists delivering exceptional care while PCPs accurately triage risk. Specialists often prefer PCPs to refer any patients who show potential signs of chronic or serious disease, rather than attempt to deliver unguided specialist-level diagnostics. Concurrently, PCPs generally want to avoid reputational risk and liability of diagnosing beyond their own base training, license, and comfort. Therefore, providing specialist guidance in the PCP office can support and affirm the diagnostics done there.
For example, asynchronous eConsults allow PCPs to get specialist advice without referring the patient to another physician. Incentives align well as patients get answers quickly, PCPs get a specialist to sign off on diagnostic triage, and specialists can review low-risk patients asynchronously. BardyDx commercialized a cardiology solution with this structure before getting acquired by Hillrom. Over time, this specialist presence and support may be augmented by AI guidance as generative AI becomes standard in PCP workflows.
PCPs are the backbone of our healthcare system, and it is increasingly important to empower them so our system can focus on health care rather than sick care. Diagnostic and procedural innovation in the PCPs’ office will require simultaneously addressing reimbursement, time, and liability concerns. We ultimately strive for quality care for the right patients, at the right time, in the right setting.
*Editor’s Note: Insight Partners has invested in Optain Health, Pictor Labs, Proscia, Medmo, Cleerly, Iterative Health, Screenpoint, Covera Health, Exacare AI, and Idoven.